The Rationale For The Use Of Bioelectronic Instrumentation In The Treatment Of Temporomandibular Dysfunction (TMD)
Why I use the K7 Evaluation System1

Initial diagnosis, whether be it in dentistry or medicine, relies greatly on information gathered from a thorough history and from comprehensive clinical examination. Choosing the correct route of treatment is based on an understanding of the pathogenesis of the disease being treated after a correct diagnosis has been confirmed subjectively and more important objectively. It has been shown repeatedly that diagnosis based on subjective evaluation alone can lead to gross errors in the diagnosis. In almost every discipline of the health care system bioelectronic instrumentation has become a paramount and necessary component to aid in the objective evaluation process. It aids in the progress and confirmation as additional hard data are obtained. This data/information will aid the doctor in arriving at a diagnosis, quantifying the parameters of the illness being treated, determining the right therapy, and evaluating therapeutic outcome. For example a cardiologist may prescribe an EKG under various condition to evaluate the stress that is being excreted on the heart.
In today's modern society it is no longer reasonable, customary, or acceptable for the physician to rely solely on history and subjective evaluation using visual examination and palpation.
Why is then that within the healthcare discipline of dentistry, with a small exception, has remained reserved and reticent to enter the age of electronic measurement/instrumentation?
Why is it that the majority of the dental professionals rely only on minimal dental radiography (if any), visual examination, audible evaluation, hand articualtion of dental models and hand manipulation of the lower jaw into a "centric relation" when it comes to the treatment of Temporomandibular Joint disorders?
Isn't the ultimate therapeutic goal for any treatment regimen to improve health by returning the body to an optimized state of physiologic comfort and function?
Scans/data are obtained pre-TENS therapy and post-TENS therapy.








 It is an electromyographical demonstration of muscle activity displaying mandibular torque. Used in the refinement of occlusal anatomy to assure balanced occlusion.
It is an electromyographical demonstration of muscle activity displaying mandibular torque. Used in the refinement of occlusal anatomy to assure balanced occlusion.
It gives an indication of:


 It is a combined recording of sagittal, frontal and lateral positioning of the mandible as it relates to the maxilla (ultimately skull) from centric occlusion over time. Scan 4/5 is the defining scan that distinguishes a NM dentist from other clinical dentists.
It is a combined recording of sagittal, frontal and lateral positioning of the mandible as it relates to the maxilla (ultimately skull) from centric occlusion over time. Scan 4/5 is the defining scan that distinguishes a NM dentist from other clinical dentists.
It gives indication of:

2) Optimized Occlusion Position, "Clinical and Scientific Validation for Optimizing the Neuromuscular Trajectory using the Chan Protocol", Clayton A. Chan D.D.S., ICCMO Anthology Vol. VII, 2005
3) Optimized Bite Protocol, "NM Bite Refinement, Level 5 K7 Practicum", Occlusion Connections, Las Vegas, NV.
In today's modern society it is no longer reasonable, customary, or acceptable for the physician to rely solely on history and subjective evaluation using visual examination and palpation.
Why is then that within the healthcare discipline of dentistry, with a small exception, has remained reserved and reticent to enter the age of electronic measurement/instrumentation?
Why is it that the majority of the dental professionals rely only on minimal dental radiography (if any), visual examination, audible evaluation, hand articualtion of dental models and hand manipulation of the lower jaw into a "centric relation" when it comes to the treatment of Temporomandibular Joint disorders?
Isn't the ultimate therapeutic goal for any treatment regimen to improve health by returning the body to an optimized state of physiologic comfort and function?
The role of Myotronics K7 Evaluation system in the objective diagnosis of TMD
The K7 Evaluation System has the capacity to record, analyze, and interpret gross and fine movements of the mandible and joint sounds, while monitoring the activity of the masticatory muscles in life time. This enables the Gneuromuscular clinician to create a measured occlusal position in the six dimension of mandibular movement with knowledge of the masticatory muscular imlication and disc/condyle relation of that particular occlusion. This philosophy abdicates from the historical philosophies of manual manipulation and hand articulation which obscured the mandibular and muscular functional implications. The use of electronic measurement assure an objective evaluation and diagnosis and assures that the created occlusion is physiologically sound. The K7 Evaluation system provides the clinician with three technologies for measuring, displaying and storing objective data on physiologic and anatomical status and function:
The primary components of TMD and the treatment modalities employed involves mandibular movement, dental occlusion, masticatory muscle and Temporomandibular Joint function. With objective data, the patient's condition before treatment can be assessed, a therapeutic plan created to effect the needed changes and the results of treatment analyzed for efficazy. Electronic instrumentation provides reproducible and quantifiable data needed for treatment.
- Jaw Tracking
- Electromyography
- Joint Sonography
The primary components of TMD and the treatment modalities employed involves mandibular movement, dental occlusion, masticatory muscle and Temporomandibular Joint function. With objective data, the patient's condition before treatment can be assessed, a therapeutic plan created to effect the needed changes and the results of treatment analyzed for efficazy. Electronic instrumentation provides reproducible and quantifiable data needed for treatment.
Jaw Tracking employing the K7 instrumentation
Mandibular tracking allows the clinician to detect and scrutinize minuscule mandibular movements in three dimensions at habitual/pathological centric occlusion and rest and compare this to post TENS (Trans Electrical Neural Stimulation) true physiologic rest position and determined Optimized Occlusal Position2 .Scans/data are obtained pre-TENS therapy and post-TENS therapy.
Pre-TENS and Post-TENS Scans
Scan 1:

It records the patient's normal opening and closing in the Sagittal and Frontal mode simultaneously.
It gives an indication of:
- Normal closure into occlusion
- Accommodated closure into occlusion
- Any interferences on the mesial/distal or buccal/lingual facing cusp inclines
- Precise terminal centric contact
- Musculo-skeletal strains
- Maximum full range of opening
Scan 2:

It is designed to record speed (velocity) of mandibular movement in both sagittal and frontal mode during opening and closing.
It gives an indication of:
- Functional joint anatomy (condyle, disc, eminence)
- Correlation between joint and occlusion
- Clicks exact location (slow down in velocity)
- Quality of terminal tooth contact
- Opening symmetry
- Occlusal stability and interferences
- Slow movements, jerky/erratic movements
- Mandibular deviations
- Muscular imbalances
- Joint health and condition
Scan 3:

It shows the three dimensional movement of the mandible of vertical, antero-posterior (AP), and lateral movements.
It gives an indication of:
- Stability of habitual REST
- Vertical position from habitual centric occlusion (CO)
- AP deviations and lateral deviations
- Muscular and joint stability/instability
- Habitual pathway of closure to terminal tooth contact
- Suggestive of possible "Clencher profile"
Scan 4 and Scan 5 are combined and taken post-TENS (it will be explained in greater detail subsequently)
Scan 6:
It shows mandibular movement during swallowing and identifies tongue activity.


It gives an indication of:
- The path of closure to centric occlusion during swallowing
- The position of the mandible during swallowing movement
- Position of the tongue during swallowing
- Lateral and anterior tongue thrust
- Occlusal stability/instability
Scan 7 resembles Scan 2 and it is taken post-TENS
Scan 8: (is also taken post-TENS and orthosis therapy)

It shows mandibular movement during functional chewing cycles.
It gives and indication of:
It gives and indication of:
- Quality of the terminal intercuspal position during function and resting mode
- Left and right lateral movement symmetry
- Measures mandibular position within the cuspal inclines
- Envelop of chewing motion
- Occlusal guarding
- Preciseness of centric terminal occlusion
- Muscle and joint health
Scan 9:

It is an EMG (Electromyograh) display of the muscle activity at postural habitual rest before TENS.
It gives and indication of:
- Showing relative resting activity/firing of masticatory and cervical muscles
- Degree of muscle accommodation during habitual REST
- Muscle hyperactivity due to malocclusion and/or fatigue
- Postural/cervical misalignments
- Clencher profiling
- Temporalis muscle and its relationship to mandibular posture
- Masseter muscle activity as it relates to tooth contact
- Cervical muscles as it relates to mandibular and head posture
- Digastric/suprahyoid muscle and its relationship to arch shape and tongue posture
Scan 10:

It is an EMG display of muscle activity post-TENS.
It gives and indication of:
- Degree of muscle relaxation at Physiologic REST
- Muscle rest due to malocclusion and/or rest
- Postural/cervical misalignments
- Clencher profiling
- Muscle recruitment
- Not all low EMG's are indication of normalcy

It is designed to record the quality of muscle recruitment of the temporalis and masseter muscles respectively during function (clenching).
It gives an indication of:
It gives an indication of:
- Quantitative display muscle activity during function
- Relative amount of work each muscle is capable of excreting
- Verify effect of orthosis therapy
- Possible occlusal imbalances
- Lack of posterior support
- Fatigued muscles vs. muscle recruitment ability
- Quality of occlusal proprioception
- Clencher profiling
- Comparison of relative muscle firing between left and right
Scan 12:

It gives an indication of:
- First tooth contact with simultaneous EMG to assist in identifying where to adjust the bite in micron levels
- Identifying diagnostically initial deflecting contacts (prematurities)
- Monitors early motor unit recruitment as the patient closes from rest position through freeway space into first tooth contact
- Allowing easy interpretation of first tooth contact
- Shows synchronous balanced muscle recruitment during closure

It is used to record mandibular range of motion including the maximum vertical opening and can be used both pre and post-TENS.
It gives an indication of:
- Level of improvement post-TENS
- Deviations and asymmetrical movements due to joint and muscle pathology
- Restrictions during maximum range of mandibular motions
- The quality of opening and closing in sagittal and frontal paths

It is a combination of jaw tracking and sonography allowing to associate sound patterns with real time opening and closing cycles of the mandible.
It gives and indication of:
- Alterations in joint tissue morphology
- Thickening of articular surface
- Macroscopic remodeling
- Condylar deviations due to articular disc displacement
- Level at which clicks occur

It gives indication of:
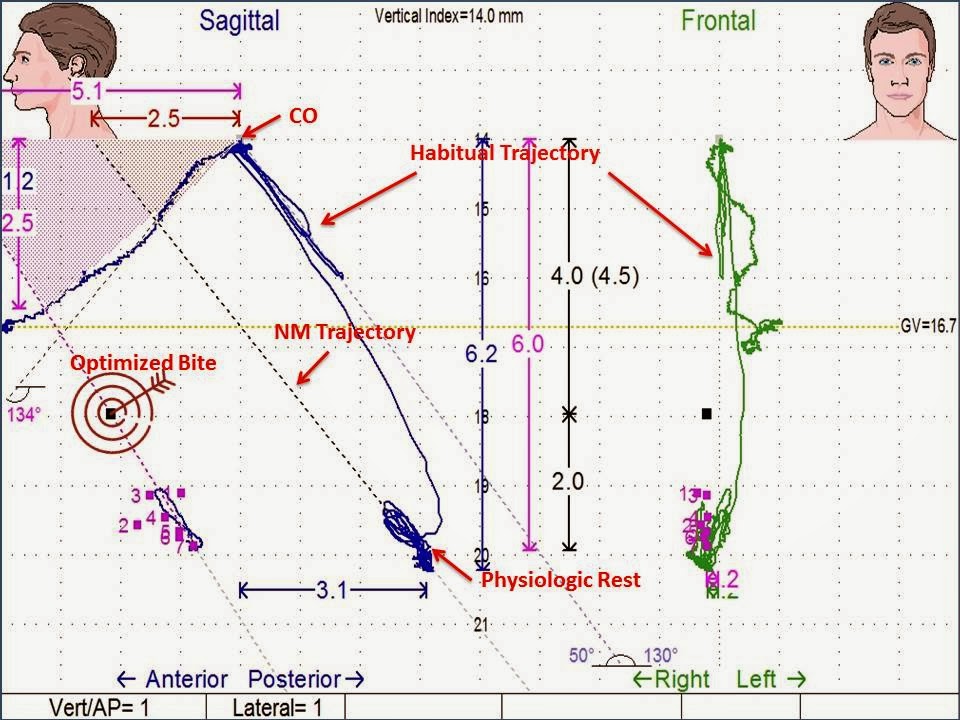
- The quality of physiologic rest after TENS
- Location habitual trajectory, the classic NM trajectory, and the Optimized trajectory
- Quality of vertical and AP pulse
- Mandibular shifts during bite recording
- Disc recapturing
- EMG recordings
- Level and stability of muscle relaxation of the masticatory and cervical system
- Repeatable
What is Bite OPTIMIZATION?
"Optimization is a term used to distinguish itself different than the classical neuromuscular jaw positioning. It is a technique and protocol that uses a systematic bite finding protocol using jaw tracking instrumentation (Myotronics K7,Scan 4/5) to “Optimize the Bite”. It is a bite recording protocol that goes beyond classical TENS bite,modified TENS bite techniques,classic scan 4/5 bite protocols and “modified Scan 4/5 bite”taking protocols developed and pioneered by the originator Dr. Clayton Chan. The Optimized Bite technique and protocol is scientific and can be measured to within 0.1-0.3 mm accuracy."Conclusion
Bioelectronic measurement instrumentation provides a road map to healthy dental occlusion, neuromuscular system and posture. It provides accurate and objective data of the mandibular and masticatory muscle function during pathology and health providing essential information for proper treatment. However, that said the clinician must develop a protocol in which each specific test adds or refines the treatment. Further the instrumentation only serves as a guide to aid in the diagnosis and treatment protocol, it is the astute clinicians knowledge to verify the data and to establish a proper outcome.
References:
1) K7 Evaluation System, Myotronics Inc. Kent, WA. USA2) Optimized Occlusion Position, "Clinical and Scientific Validation for Optimizing the Neuromuscular Trajectory using the Chan Protocol", Clayton A. Chan D.D.S., ICCMO Anthology Vol. VII, 2005
3) Optimized Bite Protocol, "NM Bite Refinement, Level 5 K7 Practicum", Occlusion Connections, Las Vegas, NV.
No comments:
Post a Comment