Neuromuscular Orthodontic approach in the treatment of Class II, pseudo Class III anterior open bite and mandibular high plane angle and the prevention of surgical intervention:
Commonly conventional orthodontics focuses on tooth to tooth relationship and a horizontal development with the teeth in habitual occlusion. To assist the progress of such a movement in a crowded, skeletal Class II situation there must be available space for this movement to take place. Standard of care in these settings dictates the extraction of four bicuspids or second molars in an adult dentition.
Further more traditional orthodontic treatment of Class II anterior open bite with high mandibular plane angle most often requires orthodontic treatment and double-jaw surgical intervention to reorient the occlusal plane toward normal. The principle of changing the occlusal plane has provided a means to improve the functional and aesthetic results for the correction of this type of facial deformity and mal-occlusion.
However, moving teeth horizontally and or surgical intervention whether extraction or double jaw surgery, does not address the functional six dimensional skeletal relationship of the mandible to the cranium (vertical, antero-posterior AP, lateral, pitch, yaw and roll), normal muscle function and normal temporo-mandibular- joint position.
Why not start from a physiologic relationship prior to orthodontic intervention?
As a dental practitioner, "physician of the mouth", it is an absolute necessity to treat all three components of the stomatognathic system to create an environment for synergistic function of teeth, temporomandibular joints and the neuromuscular system by adhering to the five principles of physiologic occlusion
1.
- Acknowledgement of the various musculoskeletal occlusal signs and symptoms
- Identification of an optimal starting point for diagnosis and treatment-"PHYSIOLOGIC REST"- without manual intervention
- Recognition of a physiologic mandibular opening and closing on a Neuromuscular Tragectory along an isotonic path for stability at a terminal contact position.
- Micro-Occlusion; eliminates the afferent and efferent noxious proprioceptive stimuli of occlusion during mandibular closure with freedom of entry and exit.
- Ability to objectively measure and record muscle and postural responses of the mandible accurately in establishing an occlusion.
One of the cardinal discoveries in the past years of research has been that there exists a six dimensional relationship of the mandible to the skull as it is dictated by the occlusal position. Any change in these six dimensions can affect the relationship of the mandible to the skull, condylar to disc relationships within the glenoid fossa of the TM joint complex, the masticatory and facial muscles, tongue position and swallowing and neck/shoulder postural balance.
Numerous musculoskeletal dysfunctions that could arise in dimensional change of mandibular/cranium relationship include:
- Headaches
- TMJ pain and noise
- Limited opening
- Vertigo (Dizziness)
- Tinnitus (Ringing in the ears)
- Dysphagia (Difficulty swallowing)
- Cervical pain
- Facial pain
- Postural problems
- Paresthesia (numbness) of fingertips
- Nervousness and insomnia
- Clenching and grinding
- Tender and sensitive teeth
- Pressure behind the eyes
It is of utmost importance before commencing with treatment that the clinician should take these signs and symptoms into consideration and be aware of the changes in mandibular/cranial relationship which could ill affect the neuromusclular and skeletal correlation.
The prevalence of skeletal distortions in these patients become apparent once the musculature is deconditioned and the neuromuscular cervical neck relationships are relaxed to allow a more accurate assessment of the mandibular/occlusal relationship to the cranium.
Necessity of objective assessment in determining a starting point:
Common fault of many clinicians is by trying to handarticulate the diagnostic casts into occlusion for establishing a reference point for treatment planning and the type of restorative, orthodontic appliance and what orthodontic treatment to implement. This has shown not to be an accurate means to determine a true physiologic dental/skeletal Class I, II, or III typing of the malocclusion. Muscle imbalance, joint pathology, mal-occlusion, worn dentition, and postural imbalances of the head, neck, shoulder and hip have shown to influence the relationship of the upper and lower jaw ultimately the relationship of the diagnostic casts. Hence, without any clear orientation and reference starting point to properly relate the study models, it makes it impossible to properly make an accurate diagnosis and decide on a proper treatment course of action and the clinician should avert relying on intuitive subjective assessment by relating the casts in a pathological bite position.
Unstable muscular functioning, joint pathology and torquing and twisting of the mandible due to sustained muscle contraction and their chronic shortening are not fully comprehended and remain undiagnosed. Electronic measurement of mandibular movement and masticatory muscle function provides invaluable objective quantitative database for diagnosing the existence and extent of myostatic contracture and skeletal malrelation. These data can then be used to design and monitor therapy and enhance treatment therapy.
K7 Myotronics: Computerized Mandibular Scanning (CMS) and Electromyography (EMG)
CMS or jaw tracking and electromyography (Myotronics, Kent, WA)2 are computerized measuring and recording instrumentation, together with an understanding of neuromuscular principles3, give clinicians the ability to provide an objective comprehensive diagnosis and allowing them to visualize jaw positioning combined with muscular responses.
Collecting objective CMS and EMG data is the first step in the analysis and understanding of mandibular movements and physiologic positioning. Interpreting the data and correlating it to clinical applications is just another step to optimal treatment outcomes.
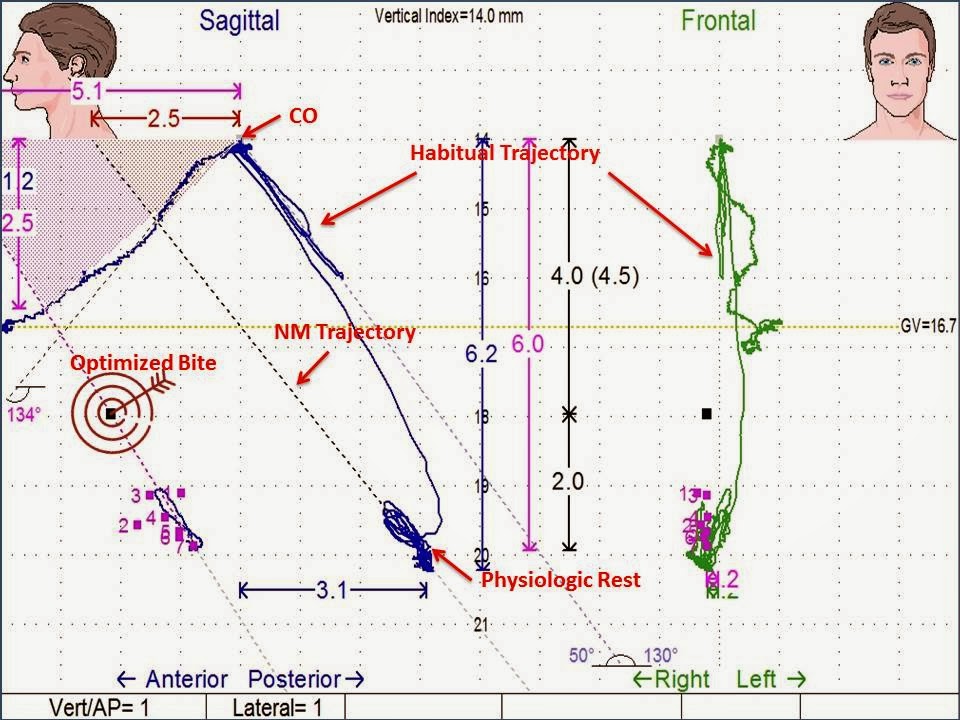
CMS measures jaw movements and locates mandibular position in space and it is displayed in a three dimensional spatial data on a computer screen. A small light weight magnet placed in the lower anterior vestibule behind the lower lip can be tracked with sensor array.
EMG measures the status of muscle by recording action potential levels of muscle pairs such as the left and right temporalis anterior, masseter, digastric and the cervical neck. These action potentials are displayed graphically pre and post treatment.
Case Study:
Neuromuscular Instrumentation used to resolve jaw mal-alignment prior to orthodontic treatment
The malocclusion with hyper divergent facial pattern or high angle are difficult to correct without combined orthodontic and orthognatic surgery approach. Treatment of patients with this type of skeletal pattern is very challenging, especially in adults who are beyond their facial growth. A surgical approach in patient who are beyond active facial growth is a viable and realistic option which permits the practitioner to attain reasonable aesthetic results and stable occlusion.
The orthopedic and orthodontic treatment of Class II high angle case requires a complete evaluation of the contributing factors.
A 39 year old female presents with severe headaches in temporal region, forehead and back of the head, amongst other symptoms. She also complained of clicking in her left and right joints, inability to open wide, and awakening with dry mouth and that she does not like the looks of her face and smile.

She was evaluated by two orthodontist and one oral surgeon who had recommended orthognatic surgical intervention and orthodontics. When evaluating and talking to patient it became apparent that the patient wanted to prevent surgical intervention at all means. This case indicates the importance of objective diagnosis and understanding of muscular limitations, joint pathology and importance of validating vertical dimension increase and its accompanying horizontal change prior to establishing a bite position to prevent misdiagnosis and treatment of jaw alignment. Using conventional tooth-to-tooth subjective orthodontics and surgical intervention to establish jaw relationships is no longer acceptable to those suffering and paining patients.
Challenges and Treatment Goals
- Identifying an optimal physiologic starting relationship between the upper and lower arches
- Muscle imbalances due to muscular pain, joint dysfunction, mal-occlusion and skeletal torques
- Advance the mandible with control of the vertical dimension
- Reduction of hyperactive muscle activity and removing the skeletal torques and skews of the jaw mal-alignment in six dimensions
- Temporomandibular Joint pathology
- Postural imbalances
- Build a stable and functional occlusion: establish Class I molar and cuspid relations with competent lips and an aesthetically pleasing smile.
Objective Assessment and Determining a Starting Point
Varying degrees of muscular dysfunction, pain and joint derangement resulting from sustained muscle contraction and chronic shortening of muscles as they pull the mandible to a pathological occlusion clearly establishes the need for being able to objectively evaluate an orthodontic case prior to commencing with treatment.
Due to these hidden implications the orthodontic clinician cannot rely on intuitive subjective determination to start treatment from hand articulating the casts in a pathological bite. This can lead to misdiagnosis and failure and relapse. Neuromuscular orthodontics emphasizes how the muscles, jaw joints and teeth affect one another and to find a physiologic relationship before aligning the teeth to one another.
Treatment Plan
In order to establish a proper treatment outcome, these cases need to be treated in two phases. Phase 1 comprises of finding the proper physiologic relationship of the mandible in six dimension and how it relates to the cranium. Establishing a starting point from where orthodontic treatment can commence. Elimination of muscle tension, patient symptoms and the achievement of a proper posture.
Phase 1:
- Radiographic series for TMJ/orthodontic, study models and pre-treatment photographs
- K7 (Myotronics Inc.) workup and TENS to establish an Optimized Bite®4
- Fabrication of a lower Gneuromuscular Orthosis
- Establish proper mandible to cranium to cervical posture
- Eliminating muscle tension and establishing a physiologic rest
- Eliminating patient symptoms
Guidelines for the fabrication of a Lower Gneuromuscular Orthopedic Repositioning Device5
The main function of an anatomical orthosis is directed toward orthopedic realignment of the mandible to the cranium, stabilizing the temporomandibular joints and return to normal physiologic function void of any craniofacial and cervical musculature strain. For the anatomical orthosis to be effective it needs to follow methodical principles of design specific to the TMJ dysfunctional patient. These design parameters are based on the four main categories of TMJ dysfunctional patients:
- Cervical Problem
- Primary TMJ Disorders
- Class II Div 2
- Anterior Open Bite
- Establishing proper maxillary and mandibular arch forms by means of expansion (if indicated)
- Level and align maxillary arch
- Incremental orthopedic vertical eruption of lower teeth and bone
- Level and align lower teeth
- Finishing which includes proper dental and skeletal Class I relationships, proper occlusion void of occlusal interferences, normal mandibular range of motion, and lack of muscle hypertonicity.
Palatal expansion was achieved by means of Max 2000 and Innovation C brackets
Case Finishing
Previous specialists were determined that this case could not be treated without surgical/orthodontic intervention. Once a physiologic bite relationship was determined, a diagnosis and treatment plan was established for proper orthodontic/orthopedic mechanics and appliance design to avoid jaw surgery. With a neuromuscular approach it was possible to objectively attain a proper mandibular relationship in six dimension and related it to the cranium. With the help of an orthosis that position was stabilized and maintained throughout the phase 2 of orthodontic/orthopedic treatment and the establishment of a proper occlusion and a Class I skeletal and dental relationship.
Summary
The right diagnosis by employing computerized measuring and recording equipment allows us to objectively identify the components of skeletal deformity and how it is being affected by mal-occlusion. As long as mal-occlusion controls the balance of the musculo-skeletal system, mandibular jaw open and closing pattern will be posterior to an isotonic path of physiologic closure. This over time will result in muscle foreshortening and eventual muscle spasm and pain. The correctness or incorrectness of the human occlusion affects the postural relationships and entities of the body system. Optimizing the mandibular position and its surrounding neuromuscular system will increase case stability and improve long term retention. Logic dictates in order to increase vertical dimension and its accompanying horizontal change in mandibular position, one has to be able to objectively verify and compare both positions in pathology and health. As health care provider we have a professional obligation to our patients and the profession of dentistry to make proper diagnosis to help bring quality dental health free of the disruptive pains of temporomandibular dysfunction to our patients.
"START WITH THE END IN MIND"
References
1. Chan C.A.: 5 Principles of Physiologic Occlusion, Level 3 Treatment Planning, Occlusion Connections, Las Vegas, NV.
2. Mytronics Inc., Kent, Wa., "Helping building the perfect bite"
3. Jankelson, R., "Neuromuscular Dental Diagnosis and Treatment", published by Ishiyaku EuroAmerica, ST Louis, MI. 2nd edition 2005
4. Chan C.A.: Optimized Bite, NM Bite Refinement Level 5 K7 Practicum, Occlusion Connections, Las Vegas, NV.
5. Chan C.A.: NM Work Up Protocol For The TMJ Dysfunctional Patient, Principles Of Physiologic Occlusion, Level 3 Treatment Planning, Occlusion Connections, Las Vegas, NV.






















































{kind=link}